Presented by: Efthymia Pavlidou MD, MSc

Edited by: Penelope Burle de Politis, MD

A 68-year-old woman presented with subacute visual loss and an iris lesion in her right eye.
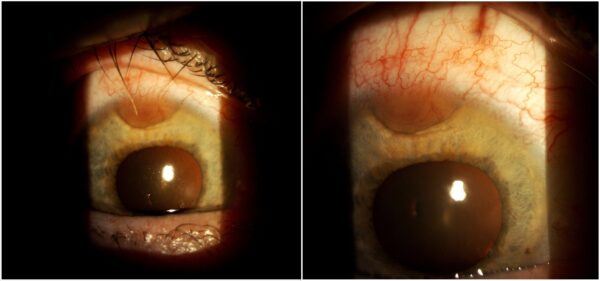
Figure 1: Slit-lamp photograph of the right eye displaying a vascularized lesion at the base of the iris, extending from 11 to 12 o’clock.
Case History
A 68-year-old Caucasian woman was referred for investigation of a superotemporal iris lesion in her right eye (RE), detected during ophthalmological examination for ipsilateral visual loss. Except for an episode of herpetic keratitis in the same eye a couple of months earlier, her past ophthalmological history was unremarkable. Her medical records included arthrosis, hypothyroidism, and a colon carcinoma treated with surgery and chemotherapy 5 years prior, with full remission according to multimodal systemic follow-up. Her family history was negative for ocular diseases. Upon examination, her best-corrected distance visual acuity (BCVA) was 4/10 in the RE and 10/10 in the left eye (LE). Refractometry was plano in the RE and +0.50 -1.00 @90° in the LE. Intraocular pressure (IOP) was 12 mmHg in the RE and 20 mmHg in the LE. Biomicroscopy showed a vascularized iris lesion in the RE, extending from 11 to 12 o’clock (Figure 1). Fundoscopy was suggestive of macular involvement in the RE. Investigation proceeded with multimodal imaging.
B-scan ultrasonography revealed that the primary lesion site was actually at the posterior chamber, with both anterior and posterior expansion (Figure 2).
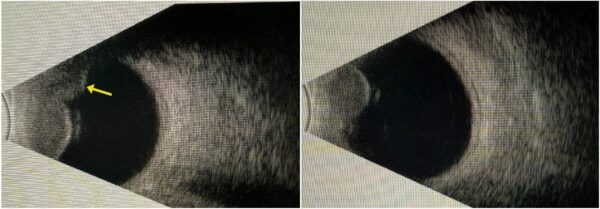
Figure 2: B-mode ultrasonography of the right eye showing a superior ciliary body mass (right), with the solid tumor pattern of low internal reflectivity (left).
Spectral-domain optical coherence tomography (SD-OCT) evidenced the presence of cystoid macular edema in the RE (Figure 3), secondary to a serous retinal detachment caused by the uveal lesion, explaining the visual deterioration in the affected eye.
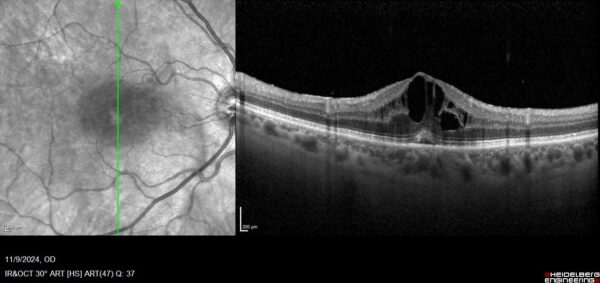
Figure 3: SD-OCT (SPECTRALIS®, Heidelberg Engineering) of the right eye demonstrating multiple hyporeflective intraretinal cysts and loss of the normal foveal contour.
Additional History
Based on the clinical presentation and multimodal imaging findings, the diagnosis of ciliary body melanoma with extension to the iris and choroid was established. Considering lesion size and contiguous invasion, enucleation was the management of choice.
The anatomopathologic analysis confirmed that the tumor arose from the ciliary body and extended posteriorly into the choroid, with significant projection into the vitreous cavity, producing focal elevation of the retina and a limited serous detachment. It also extended anteriorly into the iris, with local invasion of the Schlemm’s canal, the lens epithelium, and the sclera and cornea (sclerocorneal junction) at the limbus. Vascular infiltration was observed, but no extraocular extension was identified. The tumor measured 14.6 × 11.0 mm and its composition was mixed-cell type, with moderate mitotic activity.
Differential Diagnosis of Ciliary Body Melanoma
- primary ciliary body cyst
- melanocytoma
- iris and ciliary body leiomyoma
- granuloma
- sarcoid nodule
- adenoma of the ciliary body pigmented epithelium
- adenocarcinoma of the ciliary body pigmented epithelium
- metastatic carcinoma
The differentiation among iris-ciliary body lesions is generally based on pigmentation, vascularization, and growth rate. Transillumination is a readily available technique that helps distinguish solid from cystic growths. The classical feature of melanoma is the so-called “sentinel” vessels – dilated, tortuous episcleral blood vessels overlying the tumor.
Discussion and Literature
While uveal melanoma is the most common primary ocular malignancy in adults, affecting predominantly (97.8%) Caucasian individuals — particularly those of Northern European ancestry — tumors arising from the ciliary body comprise only about 7% of all uveal melanomas. Several predisposing factors have been identified, including light-colored iris and skin, uveal nevus, congenital ocular melanocytosis, and xeroderma pigmentosum. Multiple chromosomal abnormalities and gene mutations have been implicated in the pathogenesis of uveal melanoma. In particular, germline BAP1 mutations are associated with an increased risk of uveal melanoma and are involved in the BAP1 Tumor Predisposition Syndrome (BAP1-TPDS), which is also linked to other neoplasias, namely adenomatous colon polyposis.
Cystoid macular edema is an uncommon manifestation of uveal melanoma but may develop through several mechanisms, among which an inflammatory response to tumor necrosis or the release of tumor-related biochemical mediators into the vitreous cavity. Elevated vitreous concentrations of vascular endothelial growth factor (VEGF) have been demonstrated in eyes with choroidal melanoma, suggesting that several mechanisms may contribute to the development of macular edema in these patients.
Ciliary body melanoma is rarely diagnosed as a limited lesion, frequently extending into the choroid and/or iris before becoming clinically apparent. Patients may present with blurred vision on account of induced astigmatism or lens displacement, floaters, painless visual field loss, or ocular pain resulting from secondary angle-closure glaucoma. Dilated episcleral “sentinel” vessels are among the earliest and most characteristic signs. Another early possible finding is an unexplained reduction in IOP of at least 5 mmHg compared with the fellow eye, reflecting decreased aqueous humor production caused by disruption of the overlying ciliary epithelium. After pupillary dilation, with or without a three-mirror contact lens, the tumor may be observed as a dome-shaped mass with variable pigmentation extending toward the iris and/or posterior pole.
Melanomas of the ciliary body are often relatively large at presentation because their location behind the iris delays detection during routine ophthalmic examination. Hematogenous dissemination may occur earlier than in other uveal melanomas owing to the continuous contractions of the ciliary muscle and the rich vascular supply of the region. The average age at diagnosis ranges from 55 to 62 years, and the 10-year mortality rate is approximately 30% to 50%, primarily in consequence of metastatic dissemination. Constitutional symptoms such as weight loss, marked fatigue, persistent cough, and gastrointestinal or urinary changes may indicate systemic metastases.
Ciliary body melanomas measuring as little as 3 mm in thickness can be accurately detected by ultrasonography. Ultrasound biomicroscopy (UBM) is particularly useful for estimating tumor size and defining the anterior tumor margin. In most cases, diagnosis is based on clinical examination and imaging findings, without the need for invasive procedures. Although biopsy can provide histopathological confirmation, its role in intraocular malignancies remains controversial due to the risk of seeding malignant cells. Consequently, diagnostic biopsy is generally reserved for cases of diagnostic uncertainty, conflicting noninvasive findings, or small melanocytic lesions requiring definitive characterization.
Treatment of ciliary body melanomas depends on tumor size, local extension, and histopathological characteristics. Smaller tumors are associated with fewer complications and better visual outcomes. Surgical options range from block excision (sclerouvectomy), consisting of en bloc resection of the ciliary body, iris, cornea, and sclera with reconstruction using a lamellar scleral flap, to enucleation. Globe-preserving treatments, such as plaque brachytherapy or sclerouvectomy, may be appropriate for selected small ciliary body melanomas and choroidal melanomas near the equator. However, current evidence has not demonstrated a survival advantage of local resection over enucleation for posterior uveal melanoma. In addition, radiation therapy may result in cataract formation, punctal occlusion, keratoconjunctivitis, radiation-induced anterior uveitis, or scleral necrosis, particularly when treating large tumors. Furthermore, incomplete resection of posterior melanomas remains a concern that may favor a more radical surgical approach. On the other hand, systemic oncologic treatment, involving radiotherapy, chemotherapy, immunotherapy, targeted therapy, or palliative care, is reserved for patients with metastatic disease.
Like choroidal melanoma, ciliary body melanoma is classified according to the modified Callender classification into spindle-cell types A and B, epithelioid, mixed-cell, and necrotic subtypes. Spindle-cell melanomas generally have the most favorable prognosis, whereas epithelioid tumors, characterized by marked nuclear pleomorphism, frequent mitoses, and anaplastic features, have the poorest prognosis.
Prognostic factors include clinical features (local extension, metastatic disease, patient age), macroscopic characteristics (particularly tumor size), and microscopic findings (cell type). Tumors measuring up to 11 mm in their largest basal diameter are considered small and have an 86% five-year survival rate; those measuring 11 to 15 mm are classified as medium, with a 66% five-year survival rate, whereas tumors larger than 15 mm are considered large, with a 56% five-year survival rate. Metastatic rates are approximately 25% at 5 years and 34% at 10 years. The liver is the most common site of metastasis (95%), followed by the lungs (46%), bone (29%), and skin (17%); therefore, the initial metastatic workup should include liver function tests and chest imaging. Early detection and timely management are essential for improving clinical outcomes and life expectancy in cases of ciliary body melanoma.
Keep in mind
- Ciliary body melanoma is a rare subtype of uveal melanoma, often diagnosed late because of its location behind the iris and lack of specific symptoms.
- The diagnosis of ciliary body melanoma is based on clinical and imaging findings, not requiring diagnostic biopsy.
- Ciliary body lesions have a higher tendency to metastasize than other uveal melanomas, requiring prompt, often radical excision.
References
- Costache M, Patrascu OM, Adrian D, Costache D, Sajin M, Ungureanu E & Simionescu O (2013). Ciliary body melanoma – a particularly rare type of ocular tumor. Case report and general considerations. Maedica, 8(4), 360–364. https://pmc.ncbi.nlm.nih.gov/articles/PMC3968473
- Rogers GM, Syed NA, Alward WLM, Fernandez de Castro J & Jensen L (2010). Iris-Ciliary Body Melanoma: 57-year-old female with iris lesion. EyeRounds.org. http://www.EyeRounds.org/cases/104-Iris-Ciliary-Body-Melanoma.htm.
- Singh S, Johri P & Maurya RP (2021). Ciliary body melanoma: A case report and review of literature. IP International Journal of Ocular Oncology and Oculoplasty, 7(1), 102-104. https://doi.org/10.18231/j.ijooo.2021.022
- Riechardt AI, Kilic E & Joussen AM (2021). The Genetics of Uveal Melanoma: Overview and Clinical Relevance. Genetik der Aderhautmelanome: Übersicht und klinische Relevanz. Klinische Monatsblatter fur Augenheilkunde, 238(7), 773–780. https://doi.org/10.1055/a-1513-0789
- Jacobson AL, Roberts ME, Byrne L, Wolfe J, Stanich PP, Abdel-Rahman MH, Pritchard CC & Konnick EQ (2025). First Report of BAP1-Associated Polyposis. American journal of medical genetics. Part A, 197(12), e64176. https://doi.org/10.1002/ajmg.a.64176
- Garoon RB, Shields CL, Kaliki S & Shields JA (2012). Cystoid macular edema as the initial manifestation of choroidal melanoma. Oman journal of ophthalmology, 5(3), 187–188. https://doi.org/10.4103/0974-620X.106104
- Tigari B, Saini M, Manchanda S et al. Large ciliary body melanoma. BMJ Case Reports CP 2021;14:e246386. https://casereports.bmj.com/content/14/11/e246386
- Rusňák Š, Hecová L, Kasl Z, Sobotová M & Hauer L (2020). Uveal Melanoma Biopsy. A Review. BIOPSIE UVEÁLNÍHO MELANOMU PŘEHLED. Ceska a slovenska oftalmologie : casopis Ceske oftalmologicke spolecnosti a Slovenske oftalmologicke spolecnosti, 76(6), 247–252. https://doi.org/10.31348/2020/9
- Dogrusöz M, Jager MJ & Damato B (2017). Uveal Melanoma Treatment and Prognostication. Asia-Pacific journal of ophthalmology (Philadelphia, Pa.), 6(2), 186–196. https://doi.org/10.22608/APO.201734
- Leal Lima CC, da Fonseca MLG, Neto GH & Galvarro Vianna RN (2020). Ciliary Body Melanoma: A Case Report With A Satisfactory Clinical Evolution. JSM Ophthalmol 7(1): 1068. https://share.google/KbGzjnQOxcMQKTo3k
