Presented by: Sakellaris Dimitris, MD

Edited by: Penelope Burle de Politis, MD

A 42-year-old man presented with pain in his right eye 6 months after corneal graft surgery.
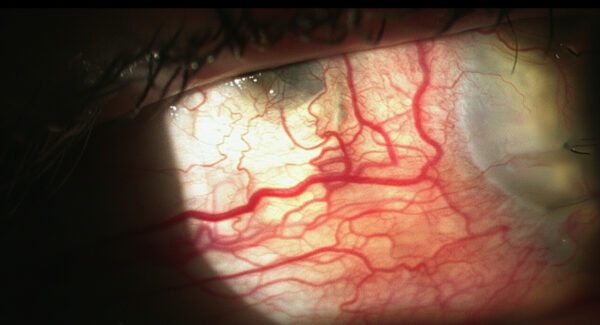
Figure 1: Slit-lamp photograph of the right eye showing congested scleral and deeper episcleral vessels and an upper temporal scleral defect.
Case History
A 42-year-old Caucasian man presented with pain in his right eye (RE) 6 months after a penetrating keratoplasty (PKP) for corneal decompensation. He had undergone bilateral cataract surgery with anterior chamber IOL implantation 17 years earlier. A Descemet’s stripping endothelial keratoplasty (DSEK) on the RE had been attempted 1 year prior to the PKP, with no satisfactory outcome. Upon examination, his best-corrected distance visual acuity (BCVA) was finger-counting in the RE and 2/10 on the left eye (LE). Corneal pachymetry was respectively 717 and 593 μm. Corrected intraocular pressure was borderline in both eyes (BE) with antiglaucomatous drops in the RE. Biomicroscopy showed congested scleral and deeper episcleral vessels and an upper temporal scleral defect (Figure 1).
The patient was started on intravenous methylprednisolone and closely monitored, with regression of the inflammatory signs over the course of one week (Figure 2).
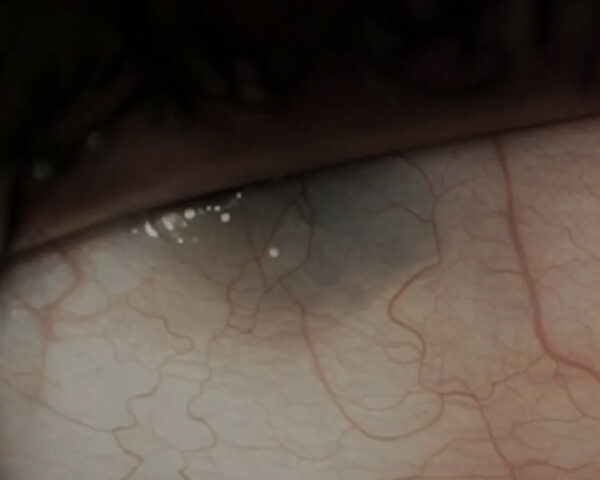
Figure 2: Slit-lamp photograph of the right eye showing a calmer ocular surface, with less congested vessels, even though the scleral lesion persists.
Additional History
The patient and 2 of his 3 children – a 17-year-old girl and a 4-year-old boy – exhibited Marfanoid features. The girl had a high stature and was pseudophakic in BE due to phacodonesis and congenital cataract. The boy presented high myopia and astigmatism (autorefractometry of -12,00D -5.50@175° in the RE and -14,50D -2.50@10° in the LE). Genetic testing for Marfan’s syndrome was recommended for the patient and his descendants.
Differential Diagnosis of Surgically-Induced Necrotizing Scleritis
● infectious scleritis
● autoimmune necrotizing scleritis
● scleromalacia
● scleral trauma
● blue sclera (congenital or acquired)
● intercalary staphyloma
Scleral necrosis and thinning may occur in association with systemic conditions or in isolation following ocular or scleral injury. Careful history and examination may help establish the etiological diagnosis for determining the appropriate approach.
Discussion and Literature
Since the 1970s, surgically-induced necrotizing scleritis (SINS) has been reported following various types of ocular surgery. There is no universally accepted nomenclature for this condition. It has also been referred to as surgically-induced scleral necrosis, postoperative scleral melting, postsurgical necrotizing scleritis, postsurgical scleral necrosis, postoperative scleral necrosis, postoperative necrotizing scleritis, and autoimmune SINS. It most often occurs after multiple ocular procedures and is believed to represent a type IV hypersensitivity reaction.
Necrotizing scleritis after ocular surgery can be defined as a progressive scleral inflammation with tissue destruction developing within the first 6 months after ocular surgery and potentially occurring even years postoperatively. Scleral disease arising as a surgical complication is most often of the necrotizing type, and necrosis is reported to be four times more common in postoperative eyes than in non-surgically induced scleritis.
Signs and symptoms of SINS include pain – sometimes associated with extraocular movement –, redness, tearing, tenderness, congestion of the deeper episcleral vessels, scleral edema, scleral necrosis, and scleral thinning or defect.
Several pathogenic mechanisms have been proposed for SINS, though they remain poorly understood. Ocular trauma may enhance the lytic activity of collagenases, with subsequent collagen degradation; vascular disruption, leading to local ischemia; and immune complex deposition with complement system activation, contributing to scleral necrosis.
It is crucial to differentiate infectious scleritis from SINS, as assuming an autoimmune etiology implies management strategies that potentiate or exacerbate primary or secondary infection, sometimes with devastating consequences. A systemic evaluation for any coexistent autoimmune disorder is advised, as 32–57% of scleritis patients have an underlying systemic disease.
Anterior segment OCT studies have shown that the anterior scleral thickness of Marfan patients is significantly lower than that of normal controls. Fibrillin, a microfibrillar glycoprotein and key component of the extracellular matrix, is the defective gene product in this condition. While abundantly present in the sclera between the collagen lamellae, the defective fibrillin may contribute to scleral thinning in affected individuals.
Regardless of the etiology of SINS, prompt treatment is essential. Non-steroidal anti-inflammatory agents are usually ineffective; therefore, immunosuppression with high dose corticosteroids – or cytotoxic agents, when necessary – should be initiated early. In case of disease progression in spite of adequate pharmacological therapy, surgical replacement of necrotic sclera may be required.
Although Marfan’s syndrome is not a recognized risk factor for necrotizing scleritis, the connective tissue fragility characteristic of Marfan patients may exacerbate scleral damage if necrotizing scleritis develops after ocular surgery.
Keep in mind
● Surgically-induced necrotizing scleritis is an idiopathic scleral necrosis that may occur months to years after one or multiple ocular surgeries.
● An immunological mechanism is likely involved in the pathogenesis of SINS and systemic autoimmune associations should be ruled out in these patients.
● Patients with Marfan’s syndrome have thinner sclerae and may be at greater risk of unfavorable outcomes in case of SINS.
References
1. Dutta Majumder P, Agarwal S, Shah M, Srinivasan B, Priyadarshini K, Iyer G, Sharma N, Biswas J & McCluskey P (2024). Necrotizing Scleritis: A Review. Ocular immunology and inflammation, 32(7), 1405–1419. https://doi.org/10.1080/09273948.2023.2206898
2. Doshi RR, Harocopos GJ, Schwab IR & Cunningham ET Jr (2013). The spectrum of postoperative scleral necrosis. Survey of ophthalmology, 58(6), 620–633. https://doi.org/10.1016/j.survophthal.2012.11.002
3. O’Donoghue E, Lightman S, Tuft S & Watson P (1992). Surgically induced necrotising sclerokeratitis (SINS)–precipitating factors and response to treatment. The British journal of ophthalmology, 76(1), 17–21. https://doi.org/10.1136/bjo.76.1.17
4. Sainz de la Maza M & Foster CS (1991). Necrotizing scleritis after ocular surgery. A clinicopathologic study. Ophthalmology, 98(11), 1720–1726. https://doi.org/10.1016/s0161-6420(91)32062-1
5. Díaz-Valle D, Benítez del Castillo JM, Castillo A, Sayagués O, Bañares A & García-Sánchez J (1998). Immunologic and clinical evaluation of postsurgical necrotizing sclerocorneal ulceration. Cornea, 17(4), 371–375. https://doi.org/10.1097/00003226-199807000-00005
6. Ruiz-Lozano RE, Garza-Garza LA, Davila-Cavazos O, Foster CS & Rodriguez-Garcia A (2021). The clinical and pathogenic spectrum of surgically-induced scleral necrosis: A review. Survey of ophthalmology, 66(4), 594–611. https://doi.org/10.1016/j.survophthal.2020.12.008
7. Magesan K, Dutta Majumder P, Agarwal M, George AE, Nair V, Ganesh SK & Biswas J (2024). Surgically induced necrotizing scleritis (SINS): Is it a standalone condition or a variant of necrotizing scleritis?. Indian journal of ophthalmology, 72(Suppl 4), S592–S595. https://doi.org/10.4103/IJO.IJO_2724_23
8. Alluyn L, Dequeker L, Dhaese S, Consejo A, De Zaeytijd J, Leroy BP, De Backer J & Kreps EO (2024). Anterior scleral thickness in Marfan’s syndrome: A quantitative analysis. Acta ophthalmologica, 102(7), e1050–e1056. https://doi.org/10.1111/aos.16721
9. Wheatley HM, Traboulsi EI, Flowers BE, Maumenee IH, Azar D, Pyeritz RE & Whittum-Hudson JA (1995). Immunohistochemical localization of fibrillin in human ocular tissues. Relevance to the Marfan’s syndrome. Archives of ophthalmology (Chicago, Ill. : 1960), 113(1), 103–109. https://doi.org/10.1001/archopht.1995.01100010105028
10. Shariati MM & Ghafari S (2025). Severe Necrotizing Anterior Scleritis in Marfan’s Syndrome: A Case of Scleromalacia Perforans. Clinical case reports, 13(10), e71138. https://doi.org/10.1002/ccr3.71138
