Presented by: Τρανός Πάρης, MD, PhD, ICOphth, FRCS

Edited by: Penelope Burle de Politis, MD

A 58-year-old man presented with an asymptomatic posterior pole mass in his left eye during routine examination.
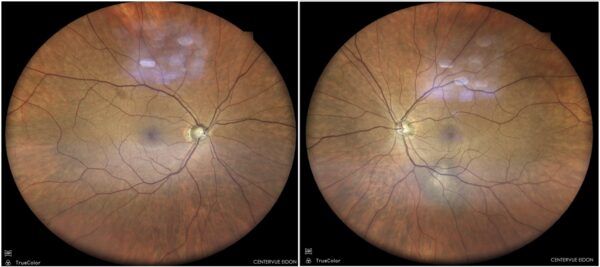
Figure 1: Color fundus photograph (EIDON TrueColor Centervue® scan) displaying an elevated slate-gray lesion along the inferior temporal arcade of the left eye, with ill-defined borders and central discoloration.
Case History
A 58-year-old Caucasian man was referred for investigation of a posterior pole elevated mass in his left eye (LE), incidentally found during a routine ophthalmologic check-up. His past ocular history was unremarkable, and his family history was negative for ocular diseases. His past medical history included systemic arterial hypertension, hypercholesterolemia, insulin-dependent diabetes mellitus, a single functional kidney, benign prostate hypertrophy, and allergy to contrast media. Upon examination, his best-corrected distance visual acuity (BCVA) was 10/10 in both eyes (BE). Refractometry was -0.50 D in the right eye (RE) and -0.75 D @130° in the LE. Intraocular pressure was within normal limits bilaterally. The anterior segment was normal and there was no relative afferent pupillary defect (RAPD) in either eye. Fundoscopy revealed an elevated slate-gray lesion along the inferior temporal arcade of the left eye, with ill-defined borders and central discoloration (Figure 1). Investigation proceeded with multimodal fundus imaging.
Spectral domain optical coherence tomography (SD-OCT) demonstrated a 526 μm-high choroidal lesion in the left eye, with 4255 μm basal diameter, but no retinal pigment epithelium (RPE) disruption (Figure 2). Scarce peripheral drusen were also noted.
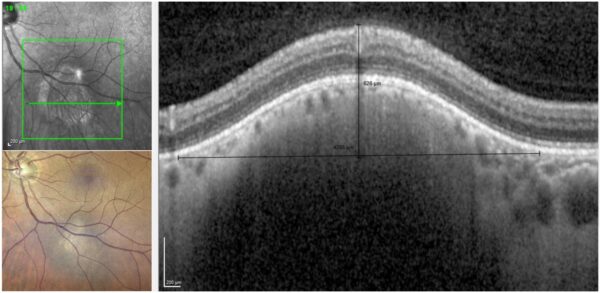
Figure 2: SD-OCT (Heidelberg Engineering®) of the left eye illustrating an elevated choroidal lesion with relative preservation of the choroidal structures, along the inferior temporal vascular arcade, in correlation with the fundus photograph.
Fundus fluorescein angiography (FFA) showed both early and late hypofluorescence of the lesion with late central staining (Figure 3).
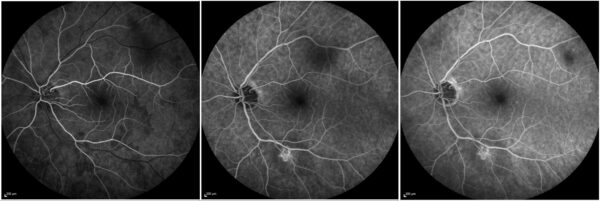
Figure 3: FFA (Heidelberg Engineering®) of the left eye showing late staining of the lesion center.
Indocyanine-green angiography (ICG-A) likewise exhibited hypofluorescence of the lesion in both early and late perfusion phases, with a focal area of hyperfluorescence (Figure 4)
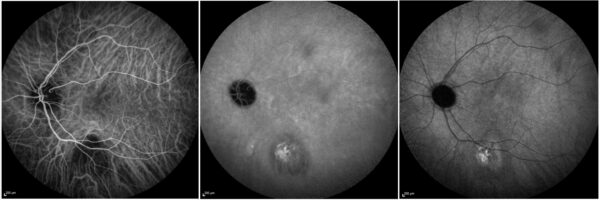
Figure 4: ICG-A (Spectralis, Heidelberg Engineering®) of the left eye showing minimal, late staining of the lesion.
Surprisingly, on OCT-angiography (OCT-A), an abnormal angiographic flow overlay was detected within the retinal tissue overlying the lesion, indicating the presence of choroidal neovascular tissue (Figure 5).
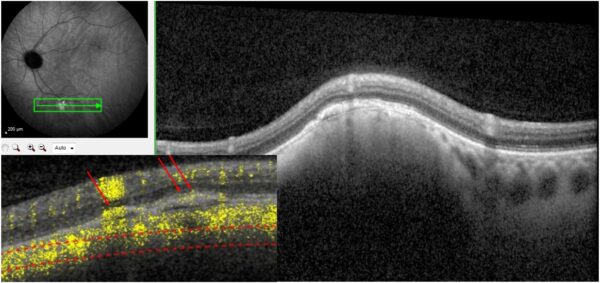
Figure 5: OCT-A (Spectralis, Heidelberg Engineering®) of the left eye depicting the abnormal flow overlay within the retinal tissue overlying the lesion.
B-scan ultrasonography displayed a thin band of moderate reflectivity at the lesion site in the posterior pole, without acoustic hollowness (Figure 6).
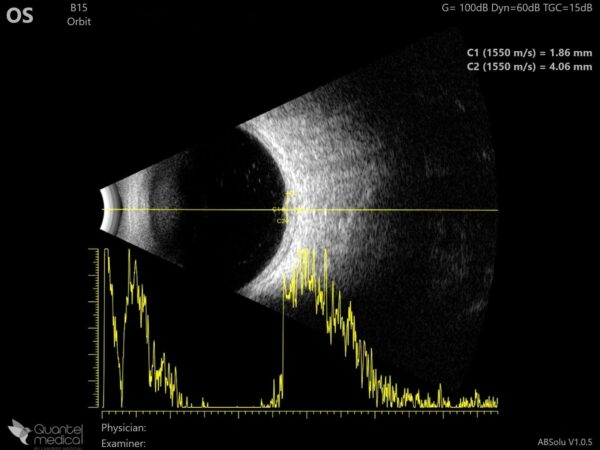
Figure 6: B-mode ultrasonogram (Quantel Medical ABSolu®) of the left eye showing relatively high and homogeneous reflectivity of the posterior pole lesion.
Additional History
At referral, the working diagnosis was choroidal hemangioma. However, the addition of multimodal imaging led to the diagnosis of choroidal nevus with neovascularization instead. Considering the lack of symptoms, the normal visual acuity, the safe distance between the lesion and the macula and optic nerve, and the quiescent appearance of the neovascularization, a conservative approach with regular follow-up was recommended.
Differential Diagnosis of Choroidal Nevus
- choroidal melanoma
- circumscribed choroidal haemangioma
- posterior scleritis
- choroidal osteoma
- choroidal metastasis
- choroidal granuloma
Different choroidal lesions can be detected on routine ophthalmological examination. Because most of them are asymptomatic and some may have a severe prognosis, fundoscopy should be performed in all patients as part of the initial ocular check-up. The differential diagnosis of choroidal lesions can be made through their particular multimodal image findings (Figure 7).
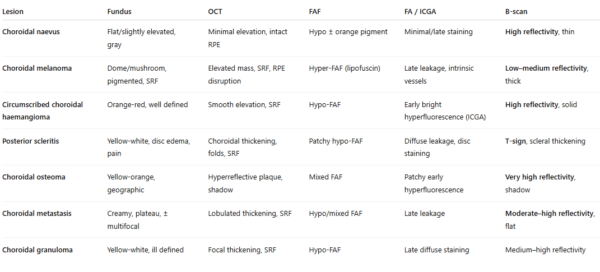
Figure 7: Comparative chart of multimodal fundus imaging features for the differential diagnosis of choroidal lesions.
Discussion and Literature
Choroidal nevi are developmental tumors and represent the most common intraocular tumor in adults. They are typically detected incidentally during routine examinations. Although the incidence of clinically detected nevi ranges from 1% to 6%, autopsy series have identified nevi in up to 9% of eyes. Caucasians are more susceptible, and there is no gender predilection. Secondary changes in the overlying retina and retinal pigment epithelium (RPE) may lead to central visual loss over time. This may occur due to several factors, including subfoveal location, RPE detachment or degeneration, foveal edema, photoreceptor degeneration, orange pigment (lipofuscin), subretinal fluid, serous retinal detachment, malignant transformation, or choroidal neovascularization (CNV). These features may lead to misinterpretation and an erroneous diagnosis of malignant transformation, although they may simply be secondary to RPE degeneration overlying the lesion or to CNV.
The clinical and histopathological findings of CNV occurring as a complication of choroidal nevi were first described by Gass in 1967. Choroidal nevus-associated CNV is uncommon, with a reported incidence of approximately 0.58% of all choroidal nevi. It is not associated with nevus size, may vary in type and location, occurs more frequently when the nevus is located in the posterior pole, and is not associated with malignant transformation – rather the opposite. Although the exact mechanisms underlying choroidal nevus-associated CNV remain incompletely understood, histopathologic studies suggest that tumor-induced damage to the choriocapillaris may play a role in its development. It has been postulated that choriocapillaris obliteration, together with a compromised mechanical barrier, promotes the release of angiogenic factors, thereby creating conditions favorable for CNV formation.
Optical coherence tomography angiography (OCT-A) is the gold-standard imaging modality for detecting choroidal nevus-associated CNV. This noninvasive technique enables visualization of both retinal and choroidal vasculature and is increasingly used for CNV detection, allowing identification of the neovascular complex both above and beneath the RPE. OCT-A is useful for delineating CNV size, shape, and location relative to a choroidal nevus, as well as for assessing choriocapillaris vascular alterations after treatment, when applicable.
The decision to treat or observe choroidal nevus-associated CNV is based on the impact of CNV on visual acuity, particularly when the lesion is juxtafoveal or subfoveal. Therapeutic options for CNV associated with choroidal nevus have included argon laser photocoagulation, verteporfin photodynamic therapy (PDT), proton beam radiotherapy (PBRT), and transpupillary thermotherapy (TTT). However, intravitreal anti-VEGF therapy is currently the preferred treatment approach.
The main concerns regarding atypical choroidal nevi are the possibility of malignant transformation and the risk of visual deterioration. Choroidal neovascularization may represent a late complication of both benign and malignant choroidal tumors; therefore, regular long-term follow-up is recommended. The combined use of multimodal imaging techniques can facilitate the detection of CNV associated with choroidal nevus and guide timely treatment to preserve visual acuity.
Keep in mind
- CNV is a rare complication of choroidal nevi, the most common intraocular tumour.
- The diagnosis of choroidal nevus-associated CNV can be guided by multimodal fundus imaging.
- Intravitreal anti-VEGF therapy is the treatment of choice for vision-threatening CNV associated with choroidal nevus.
References
- Papastefanou VP, Nogueira V, Hay G, Andrews RM, Harris M, Cohen VM & Sagoo MS (2013). Choroidal naevi complicated by choroidal neovascular membrane and outer retinal tubulation. The British journal of ophthalmology, 97(8), 1014–1019. https://doi.org/10.1136/bjophthalmol-2013-303234
- Callanan DG, Lewis ML, Byrne SF & Gass JD (1993). Choroidal neovascularization associated with choroidal nevi. Archives of ophthalmology (Chicago, Ill. : 1960), 111(6), 789–794. https://doi.org/10.1001/archopht.1993.01090060077026
- Zografos L, Mantel I & Schalenbourg A (2004). Subretinal choroidal neovascularization associated with choroidal nevus. European journal of ophthalmology, 14(2), 123–131. https://doi.org/10.1177/112067210401400207
- Novais EA, Adhi M, Moult EM, Louzada RN, Cole ED, Husvogt L, Lee B, Dang S, Regatieri CV, Witkin AJ, Baumal CR, Hornegger J, Jayaraman V, Fujimoto JG, Duker JS & Waheed NK (2016). Choroidal Neovascularization Analyzed on Ultrahigh-Speed Swept-Source Optical Coherence Tomography Angiography Compared to Spectral-Domain Optical Coherence Tomography Angiography. American journal of ophthalmology, 164, 80–88. https://doi.org/10.1016/j.ajo.2016.01.011
- Di Staso F, Di Pippo M & Abdolrahimzadeh S (2023). Choroidal Neovascular Membranes in Retinal and Choroidal Tumors: Origins, Mechanisms, and Effects. International journal of molecular sciences, 24(2), 1064. https://doi.org/10.3390/ijms24021064
- Pellegrini M, Corvi F, Say EAT, Shields CL & Staurenghi G (2018). OPTICAL COHERENCE TOMOGRAPHY ANGIOGRAPHY FEATURES OF CHOROIDAL NEOVASCULARIZATION ASSOCIATED WITH CHOROIDAL NEVUS. Retina (Philadelphia, Pa.), 38(7), 1338–1346. https://doi.org/10.1097/IAE.0000000000001730
- Cennamo G, Montorio D, Fossataro F, Clemente L, Carandente R & Tranfa F (2021). Optical coherence tomography angiography in quiescent choroidal neovascularization associated with choroidal nevus: 5 years follow-up. European journal of ophthalmology, 31(5), NP111–NP115. https://doi.org/10.1177/1120672120934390
- Chiang A, Bianciotto C, Maguire JI, Park CH, Baker PS, Shields JA & Shields CL (2012). Intravitreal bevacizumab for choroidal neovascularization associated with choroidal nevus. Retina (Philadelphia, Pa.), 32(1), 60–67. https://doi.org/10.1097/IAE.0b013e31822092b7
- Cavalcante ML, Villegas VM, Gold AS, Cavalcante LL, Lonngi M, Shah NV & Murray TG (2014). Treatment of vascular activity secondary to atypical choroidal nevus using intravitreal bevacizumab. Clinical ophthalmology (Auckland, N.Z.), 8, 1377–1382. https://doi.org/10.2147/OPTH.S64138
- D’andrea L, Fossataro F & Cennamo G (2020). Choriocapillary vascular density changes in choroidal neovascularization associated with choroidal nevus after anti-VEGF injections. European journal of ophthalmology, 1120672120982946. Advance online publication. https://doi.org/10.1177/1120672120982946
